Hearing Reconstruction Cases
Ossicular Chain Reconstruction Case Number 1
This patient had undergone significant TMJ surgery. During the surgery, she sustained damage to her ear canal and eardrum, with resultant perforation of the eardrum and conductive hearing loss. She was found to have damage to the 2nd and 3rd hearing bones, the incus and the stapes. These were reconstructed and her eardrum repaired.

A wispy perforation of the eardrum is seen.
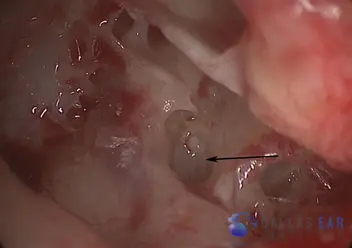
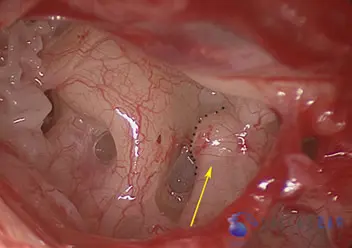
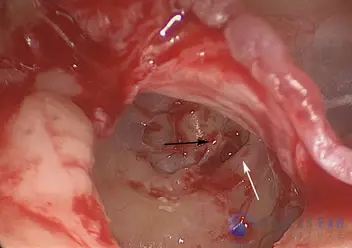
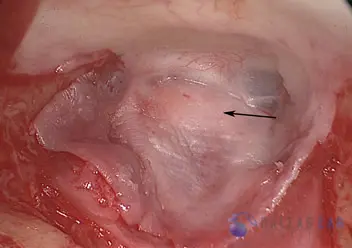
The eardrum is elevated and the middle ear is explored. The arrow signifies the footplate, which is the mobile barrier between the inner ear and the middle ear. Typically, the stapes, or 3rd hearing bone, sits on top of this footplate and vibrates the the fluid of the inner ear to create hearing. In this ear, there is no connection between the eardrum and the inner ear because the hearing bones are completely missing from the previous damage she sustained.

This is a titanium shoe that will sit on the footplate and will accept the prosthesis into it.

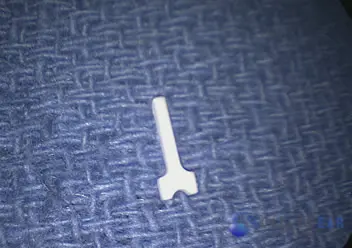
This is a titanium and hydroxyapatite prosthesis that will connect the eardrum to the inner ear. The length of this prosthesis is about 5 mm. This prosthesis will fit into the footplate shoe (previous image) and allow vibration of the footplate and inner ear fluid so that hearing can occur.
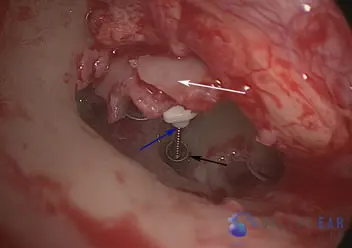
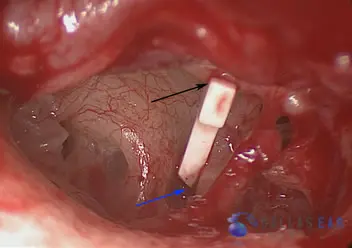
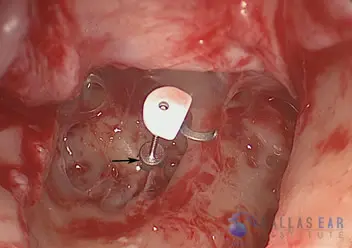
The prosthesis is placed into the middle ear to allow hearing. The titanium footplate shoe (black arrow) sits on top of the footplate. The hearing prosthesis bridges the gap between the eardrum and the inner ear (blue arrow). A cartilage graft (white arrow) is placed on top of the prosthesis to stabilize it in the middle ear and to prevent it from extruding through the eardrum.
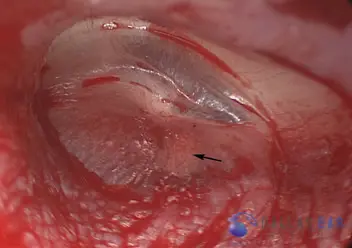
The eardrum perforation is repaired (black arrow) and the ear canal is packed with dissolvable packing to allow healing. Her hearing is immediately improved with this procedure.
Ossicular Chain Reconstruction Case Number 2
This 30-year-old patient presented with a hearing loss in his left ear that he had noted since he was a child. He recounted a history of multiple ear infections and head trauma to the left side as a child, and a severe hearing loss in the ear for many years. Upon exploring his middle ear, he was found to lack the incus and stapes hearing bones (the 2nd and 3rd hearing bones), and this explained his severe hearing loss. In addition, he was found to have a significant dehiscence of his facial nerve—the bone that typically covers his facial nerve (the nerve supplies all of the muscles of the face) was completely gone and the nerve was exposed. The nerve was not disturbed, and his hearing was completely restored by reconstructing the ossicular chain.

The eardrum looks completely normal and healthy. As you can see, the first hearing bone (black arrow) is attached to the eardrum, as is the case in normal ears.
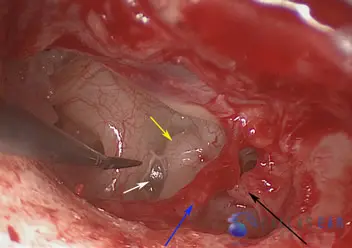
The eardrum has been elevated and a view of the middle ear is obtained. Access is gained to the tiny hearing bones of the middle ear by making a small incision in the ear canal and lifting the eardrum forward. The blue arrow signifies the chorda tympani nerve, which is a taste nerve that runs through the middle ear. This nerve is not disturbed during this surgery. The black arrow is pointing towards the remnant of the incus, or 2nd hearing bone. This bone has been nearly completely eroded—the only part that is left of the bone is the head of the incus, which the black arrow is pointing towards. The white arrow is pointing towards the stapes footplate. In a normal ear, the stapes bone (3rd hearing bone that is shaped like a horseshoe) sits on top of this plate that separates the middle ear from the inner ear. Motion of this bone on this footplate allows us to hear. In this case, the bone is completely gone and there is no connection between the eardrum and the inner ear. Lastly, the facial nerve that runs above the stapes footplate lacks the bone that typically covers this nerve. The yellow arrow indicates a “knuckle” in the nerve that is protruding down.
This image shows the facial nerve and the dehiscence, or exposure, of the nerve in the middle ear cavity.
This is a prosthesis that will reconnect the eardrum and the inner ear, allowing hearing recovery. This is trimmed to the correct size and placed in the middle ear to re-establish the normal function of the ear.
The prosthesis is placed from the malleus, or 1st hearing bone, to the footplate of the inner ear. Now, movement of the eardrum from sound will vibrate the footplate and allow hearing to occur.
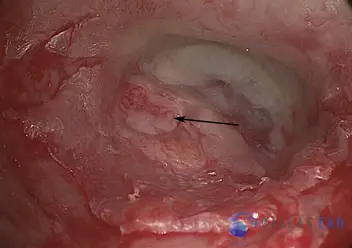
The eardrum is replaced. A faint shadow of the prosthesis is visible through the eardrum (black arrow). This prosthesis will stay in place and should afford hearing for the rest of the patient’s life.
Ossicular Chain Reconstruction Case Number 3
This patient has had several ear surgeries in her past when she was a young child. Her eardrum is very lateralized—it has healed into place too far out in the ear canal. Her hearing is very poor with a large conductive hearing loss. After considering options, she elected to proceed with a middle ear exploration and assessment of her hearing mechanism.

The eardrum is noted to be laterally displaced. It is intact. There are no ossicular elements noted.
The stapes bone (black arrow) is clearly visualized once the eardrum is elevated. There is no connection between the eardrum and the stapes, the third hearing bone. Thus, this patient had a maximal conductive hearing loss. The white arrow is pointing towards the facial nerve, that lies just above the stapes bone.
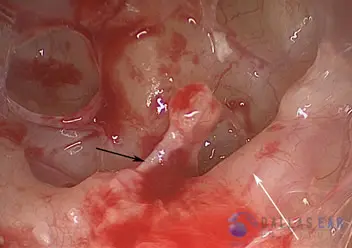
A close-up view of the stapes bone and the facial nerve (white arrow). The black arrow signifies the stapedius muscle that is attached to the stapes bone and serves a functional role. When a very loud sound enters the ear, this muscle contracts, stiffening the stapes bone and limits the amount of motion of the stapes bone and decreases potential damage to the inner ear.
Hearing reconstruction is begun by placing a prosthesis over the stapes bone (black arrow). This implant replaced the 2nd hearing bone, thus connecting the eardrum to the 3rd hearing bone and thus the inner ear. This prosthesis has a titanium basket that rests on the mobile stapes bone.
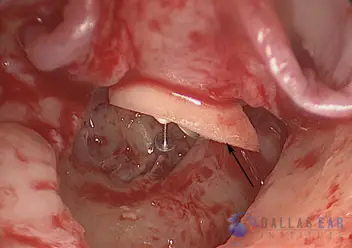
A cartilage graft is taken from the tragus cartilage of the ear. The cartilage is shaved and placed over the prosthesis and under the eardrum. This shell of cartilage sits atop the implant, stabilizing it within the middle ear and also preventing extrusion of the implant through the eardrum.
The eardrum is then placed into position, over the cartilage graft and the prosthesis. The black arrow shows the cartilage graft that is barely visualized through the eardrum. Now, when sound enters the ear canal, it will vibrate the eardrum, thus moving the prosthesis that was placed on the stapes bone and allowing the patient to hear.