Semicircular Canal Occlusion
Surgical Procedure for BPPV:
In a minority of patients with BPPV, probably less than 5%, BPPV cannot be adequately controlled with particle-repositioning maneuvers, Brandt-Daroff exercises or even customized vestibular rehabilitation therapy. In such instances surgery may be indicated. Surgery cannot be undertaken for BPPV unless the correct ear and affected canal have been reliably identified. Surgery has only been described for the posterior semicircular canal, the most commonly affected. In theory, other canals could potentially be addressed, but the risks of hearing loss might be greater in certain circumstances.
The simplest and most reliable surgery is mechanical occlusion of the affected posterior semicircular canal. The canal is exposed via a mastoidectomy, drilling the bone behind the ear, and it is gently opened up and occluded with bone dust and/or other materials. In properly selected patients this procedure will be successful the vast majority of times. Recovery is typically rapid. Some motion-related imbalance may be experienced for a few weeks as the brain recovers from the loss of function from the one canal, but this is usually minor. There can also be a mild degree of hearing loss after the surgery, though this is usually temporary. There is a risk of permanent hearing loss associated with this procedure, though this is rare.
Posterior Semicircular Canal Occlusion Case
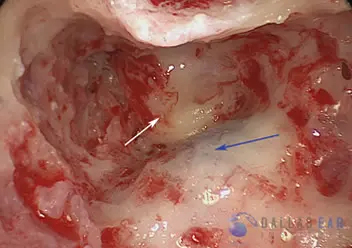
The mastoid cavity is exposed. This is accomplished by making an incision behind the ear and using a drill to open the honey-comb mastoid bone. The blue arrow indicates the sigmoid sinus, which is the continuation of the jugular vein from the neck. The white arrow is pointing toward the solid bone of the inner ear. This is clearly seen to be much more dense than the mastoid bone. The balance canals are housed in this bone.
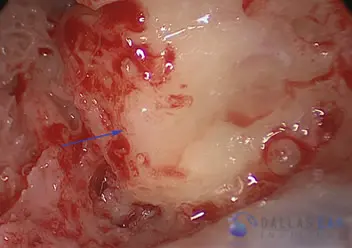
A close-up view of the dense bone of the inner ear. The mastoid air cells surrounding the inner ear structures are removed to gain access to the balance canals.
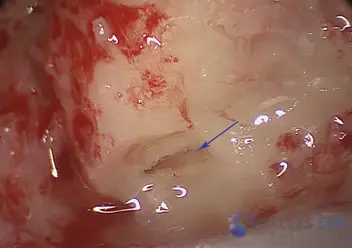
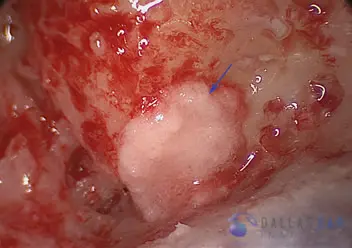
An opening is created into the bony posterior balance canal (blue arrow). There are three balance canals in each inner ear: the superior, horizontal, and posterior semicircular canal. The canal is exposed so that the procedure may be completed.
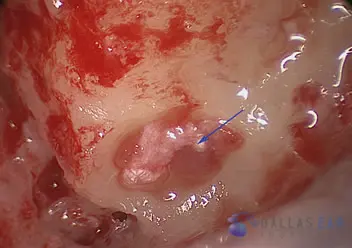
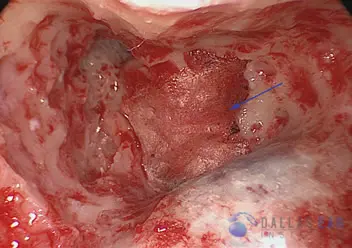
A small plug of fascia, the thin tissue layer that surrounds the muscle behind the ear, is placed into the posterior semicircular canal (blue arrow). Gently inserting this fascia into the balance canal occludes, or plugs, this canal and prevents the symptoms of Benign Paroxysmal Positional Vertigo.
Tiny bone chips taken during the drilling process are then placed over the posterior semicircular canal and the fascia plug to enhance the occlusion of the canal.
A dry fascia graft is then placed over the repair as another layer of support. The skin incision is then closed and the procedure is completed.